KENNEDY JFK ASSASSINATION MEDICAL TREATMENT HEAD THROAT WOUNDS WARREN AUTOPSY REPORT,
THE GRAND SUBVERSION:Parkland Hospital Dallas Doctors - Head, Throat gunshot Wound Description JFK Assassination Shots. |
|
|
| Parkland Hospital Witnesses | Parkland Head Wound | |
| Parkland Throat Wound | ||
|
Autopsy Page ( 3 )
|
Grandsubversion.com:
SECTION:
[Parkland Hospital]--[Bethesda
Autopsy]--[Dallas I]--[Dallas
II]--[Shots]--[Magic
Single Bullet Theory]--[Oswald
I]--[Oswald II]--[Oswald
III]--[Oswald
IV]--[Three
Tramps]--[Dallas
Police]
PARKLAND HOSPITAL, HEAD WOUND medical Description:
Dr.
Akin -
Dr.
Bashour -
Dr.
Baxter -
Nurse
Bowron -
Dr.
Carrico -
Dr.
Clark - Dr.
Giesecke -
Dr.
Jenkins - Dr.
Jones
- Dr.
McClelland - Dr.
Perry
- Dr.
Peters - Dr.
Salyer
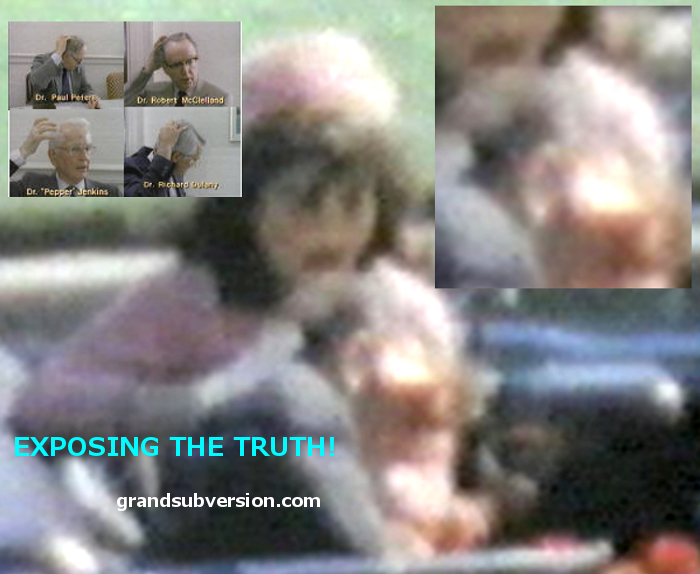
Parkland Hospital Dallas Doctors, JFK
Assassination: HEAD SHOT PHOTO.
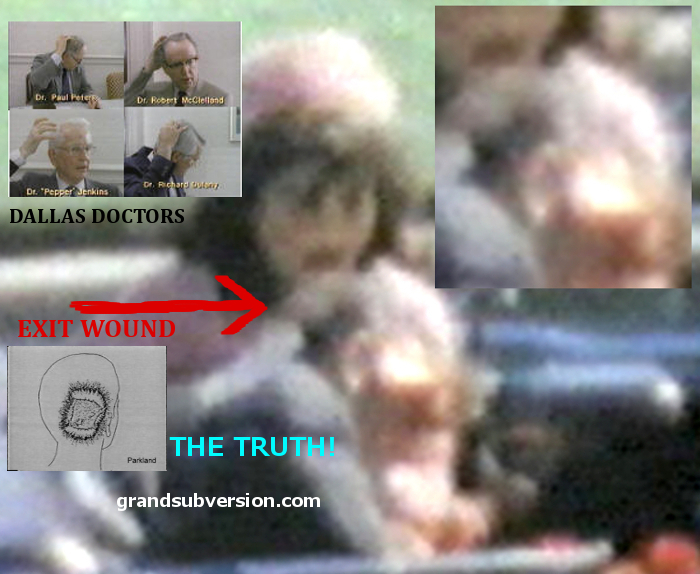
HEAD SHOT PHOTO CLOSE UP JFK KENNEDY ZAPRUDER FILM FRAME HEAD WOUND.
DR. Gene Coleman Akin, Anesthesiology.:
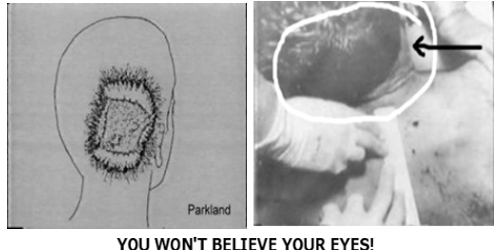
"The back of the right occipitalparietal portion of his head was shattered, with
brain substance extruding."
Dr. Fouad Bashour, cardiology:
"The President was lying on the stretcher, the head wound was massive, the blood
was dripping from the head, and at that time the President had an endotracheal
tube."
Dr. Charles Rufus Baxter, general surgeon:
"There was a large gaping wound in the skull which was covered at that time with
blood, and its extent was not immediately determined."
*** "we had an opportunity to look at his head wound then and saw that the
damage was beyond hope, that is, in a word-- literally the right side of his
head had been blown off. With this and the observation that the cerebellum was
present--a large quantity of brain was present on the cart."
*** "The only wound that I actually saw--Dr. Clark examined this above the
manubrium of the sternum, the sternal notch. This wound was in temporal parietal
plate of bone laid outward to the side and there was a large area, oh, I would
say 6 by 8 or 10 cm. of lacerated brain oozing from this wound."
Mr. SPECTER. Did you notice any bullet hole below that large opening at the top
of the head?
Dr. BAXTER. No; I personally did not.
▲
▲
Diana Bowron, registered nurse:
Mr. SPECTER. And what, in a general way, did you observe with respect to
President Kennedy's condition?
Miss BOWRON. He was very pale, he was lying across Mrs. Kennedy's knee and there
seemed to be blood everywhere. When I went around to the other side of the car I
saw the condition of his head.
Mr. SPECTER. You saw the condition of his what?
Miss BOWRON.
The back of his head.
Mr. SPECTER. And what was that condition?
Miss BOWRON.
Well, it was very bad---you know.
Mr. SPECTER. How many holes did you see?
Miss BOWRON. I just saw one large hole.
Mr. SPECTER. Did you see a small bullet hole beneath that one large hole?
Miss BOWRON. No, sir.
Mr. SPECTER. Did you notice any other wound on the President's body?
Miss BOWRON. No, sir.
▲
▲
Dr. Charles James Carrico, surgery:
Mr. SPECTER. Will you describe as specifically as you can the head wound which
you have already mentioned briefly?
Dr. CARRICO. Sure.
This was a 5- by 71-cm defect in the posterior skull, the occipital region. There was an absence of the calvarium or skull in this area,
with shredded tissue, brain tissue present and initially considerable slow
oozing. Then after we established some circulation there was more profuse
bleeding from this wound.
Mr. SPECTER. Was any other wound observed on the head in addition to this large
opening where the skull was absent?
Dr. CARRICO. No other wound on the head.
Mr. SPECTER. Did you have any opportunity specifically to look for a small wound
which was below the large opening of the skull on the right side of the head?
Dr. CARRICO. No, sir; ***
Dr. William Kemp Clark, neurological Surgeon:
"I then examined the wound in the back of the President's head.
This was a large, gaping wound in the right posterior
part, with cerebral and cerebellar
tissue being damaged and exposed."
***
Mr. SPECTER. What, if anything, did you say then in the course of that press
conference ?
Dr. CLARK. I described the President's wound in his head in very much the same
way as I have described it here. I was asked if this wound was an entrance
wound, an exit wound, or what, and I said it could be an exit wound, but I felt
it was a tangential wound.
Mr. SPECTER. Which wound did you refer to at this time ?
Dr. CLARK. The wound in the head.
Mr. SPECTER. Did you describe at that time what you meant by "tangential"?
Dr. CLARK. Yes, sir; I did.
Mr. SPECTER. What definition of "tangential" did you make at that time?
Dr. CLARK. As I remember, I defined the word "tangential" as being---striking an
object obliquely, not squarely or head on.
Mr. SPECTER. Will you describe at this time in somewhat greater detail the
consequences of a tangential wound as contrasted with another type of a striking
?
***
Dr. CLARK. The effects of any missile striking an organ or a function of the
energy which is shed by the missile in passing through this organ when a bullet
strikes the head, if it is able to pass through rapidly without shedding any
energy into the brain, little damage results, other than that part of the brain
which is directly penetrated by the missile. However, if it strikes the skull at
an angle, it must then penetrate much more bone than normal, therefore, is
likely to shed more energy, striking the brain a more powerful blow. Secondly,
in striking the bone in this manner, it may cause pieces of the bone to be blown
into the brain and thus act as secondary missiles. Finally, the bullet itself
may be deformed and deflected so that it would go through or penetrate parts of
the brain, not in the usual direct line it was proceeding.
***
Mr. SPECTER Now, you described the massive wound at the top of the President's
head, with the brain protruding; did you observe any other hole or wound on the
President's head?
Dr. CLARK. No, sir; I did not.
Mr. SPECTER. Did you observe, to make my question very specific, a bullet hole
or what appeared to be a bullet hole in the posterior scalp, approximately 2.5
cm. laterally to the right, slightly above the external occipital protuberant,
measuring 15 by 6 mm.
Dr. CLARK. No, sir; I did not. This could easily have been hidden in the blood
and hair.
Mr. SPECTER. Did you observe any bullet wounds or any other wound on the back
side of the President?
Dr. CLARK. No, sir; I did not.
***
Mr. SPECTER. Dr. Clark, would your observations be consistent with some other
alleged facts in this matter, such as the presence of a lateral wound measuring
15 by 6 mm. on the posterior scalp approximately 2.5 cm. laterally to the right
and slightly above the external occipital proturberant--that is to say, could
such a hole have been present without your observing it?
Dr. CLARK. Yes, in the presence of this much destruction of skull and scalp
above such a wound and lateral to it and the brief period of time available for
examination--yes, such a wound could be present.
▲
▲
Dr. Adolph Hartung Giesecke, Jr, anesthesiology:
As I moved around towards the head of the emergency cart with the anesthesia
machine and the resuscitative equipment and helped Dr. Jenkins to hook the
anesthesia machine up to the President to give him oxygen, I noticed that he had
a very large cranial wound, with loss of brain substance, and it seemed that
most of the bleeding was coming from the cranial wound.
Mr. SPECTER. What did you observe specifically as to the nature of the cranial
wound ?
Dr. GIESECKE. It seemed that from the vertex to the left ear, and from the browline to the occiput on the left-hand side of the head the cranium was
entirely missing.
Mr. SPECTER. Was that the left-hand side of the head, or the right-hand side of
the head ?
Dr. GIESECKE. I would say the left, but this is just my memory of it.
Mr. SPECTER. That's your recollection ?
Dr. GIESECKE. Right, like I say, I was there a very short time really.
Mr. SPECTER. Did you observe any other wound or bullet hole below the large area
of missing skull ?
Dr. GIESECKE. No; when I arrived the tracheotomy was in progress at that time
and so I observed no other wound except the one on the cranium.
Mr. SPECTER. On the cranium itself, did you observe another bullet hole below
the portion of missing skull ?
Dr. GIESECKE. No, sir; this was found later by Dr. Clark--I didn't see this.
Mr. SPECTER. What makes you say that that hole was found later by Dr. Clark?
Dr. GIESECKE. Well, this is hearsay--I wasn't there when they found it and I
didn't notice it.
Mr. SPECTER. Well, Dr. Clark didn't observe that hole.
Dr. GIESECKE. Oh, he didn't--I'm sorry.
Mr. SPECTER. From whom did you hear that the hole had been observed, if you
recollect?
Dr. GIESECKE-. Oh--I must be confused. We talked to so many people about these
things--I don't remember.
▲
▲
Dr. Marion Thomas Jenkins, Anesthesiology:
Mr. SPECTER. Now, will you now describe the wound which you observed in the
head?
Dr. JENKINS. Almost by the time I was--had the time to pay more attention to the
wound in the head, all of these other activities were under way. I was busy
connecting up an apparatus to respire for the patient, exerting manual pressure
on the breathing bag or anesthesia apparatus, trying to feel for a pulse in the
neck, and then reaching up and feeling for one in the temporal area, seeing
about connecting the cardioscope or directing its being connected, and then
turned attention to the wound in the head. Now, Dr. Clark had begun closed chest
cardiac massage at this time and I was aware of the magnitude of the wound,
because with each compression of the chest, there was a great rush of blood from
the skull wound. Part of the brain was herniated; I really think part of the
cerebellum, as I recognized it, was herniated from the wound; there was part of
the brain tissue, broken fragments of the brain tissue on the drapes of the cart
on which the President lay.
Mr. SPECTER. Did you observe any wounds immediately below the massive loss of
skull which you have described?
Dr. JENKINS. On the right side?
Mr. SPECTER. Yes, sir.
Dr. JENKINS. No---I don't know whether this is right or not, but I thought there
was a wound on the left temporal area, right in the hairline and right above the
zygomatic process.
Mr. SPECTER. The autopsy report discloses no such development, Dr. Jenkins.
Dr. JENKINS. Well, I was feeling for---I was palpating here for a pulse to see
whether the closed chest cardiac massage was effective or not and this probably
was some blood that had come from the other point and so I thought there was a
wound there also.
▲
▲
Dr. Ronald Coy Jones, General Surgery:
Mr. SPECTER. Will you describe as precisely as you can the nature of the head
wound ?
Dr. JONES.
There was large defect in the back side of the head as the President
lay on the cart with what appeared to be some brain hanging out of this wound
with multiple pieces of skull noted next with the brain and with a tremendous
amount of clot and blood.
***
Mr. SPECTER. Have you ever had any formal training in bullet wounds?
Dr. JONES. No.
Mr. SPECTER. Have you ever had occasion to observe a bullet wound which was
inflicted by a missile at approximate size of a 6.5 ram. bullet which passed
through the body of a person and exited from a neck without striking anything
but soft tissue from the back through the neck, where the missile came from a
weapon of the muzzle velocity of 2,000 feet per second, and the victim was in
the vicinity of 160 to 250 feet from the weapon?
Dr. JONES. No; I have not seen a missile of this velocity exit in the anterior
portion of the neck. I have seen it in other places of the body, but not in the
neck.
Mr. SPECTER. What other places in the body have you seen it, Dr. Jones?
Dr. JONES. I have seen it in the extremity and here it produces a massive amount
of soft tissue destruction.
Mr. SPECTER. Is that in the situation of struck bone or not struck bone or what?
Dr. JONES. Probably where it has struck bone.
Mr. SPECTER. In a situation where it strikes bone, however, the bone becomes so
to speak a secondary missile, does it not, in accentuating the soft tissue
damage?
Dr. JONES. Yes.
Mr. SPECTER. Dr. Jones, did you have any speculative thought as to accounting
for the point of wounds which you observed on the President, as you thought
about it when you were treating the President that day, or shortly thereafter?
Dr. JONES. With no history as to the number of times that the President had been
shot or knowing the direction from which he had been shot, and seeing the wound
in the midline of the neck, and what appeared to be an exit wound in the
posterior portion of the skull, the only speculation that I could have as far as
to how this could occur with a single wound would be that would enter the
anterior neck and possibly strike a vertebral body and then change its course
and exit in the region of the posterior portion of the head. However, this
was--there was some doubt that a missile that appeared to be of this high
velocity would suddenly change its course by striking, but at the present-at
that time, if I accounted for it on the basis of one shot, that would have been
the way I accounted for it.
Mr. SPECTER. And would that account take into consideration the extensive damage
done to the top of the President's head ?
Dr. JONES. If this were the course of the missile, it probably--possibly could
have accounted for it, although I would possibly expect it to do a tremendous
amount of damage to the vertebral column that it hit and if this were a high
velocity missile would also think that the entrance wound would probably be
larger than the one that was present at the time we saw
Mr. SPECTER. Did you observe whether or not there was any damage to the
vertebral column ?
Dr. JONES. No, we could not see this.
Mr. SPECTER. Did you discuss this theory with any other doctor or doctors?
Dr. JONES. Yes; this was discussed after the assassination.
Mr. SPECTER. With whom ?
Dr. JONES. With Dr. Perry--is the only one that I recall specifically, and that
was merely as to how many times the President was shot, because even immediately
after death, within a matter of 30 minutes, the possibility of a second gunshot
wound was entertained and that possibly he had been shot more than once.
▲
▲
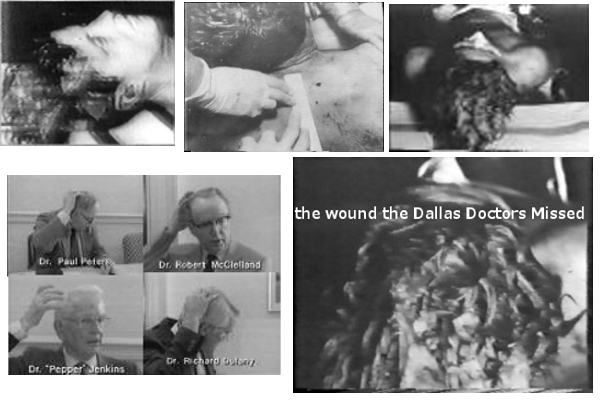
Dr. Robert Nelson McClelland, general surgery:
Mr. SPECTER. Before proceeding to describe what you did in connection with the
tracheostomy, will you more fully describe your observation with respect to the
head wound?
Dr. MCCLELLAND. As I took the position at the head of the table that I have
already described, to help out with the tracheotomy,
I was in such a position
that I could very closely examine the head wound, and I noted that the
right
posterior portion of the skull had been extremely blasted. It had been
shattered, apparently, by the force of the shot so that the parietal bone was
protruded up through the scalp and seemed to be fractured almost along its right
posterior half, as well as some of the occipital bone being fractured in its
lateral haft, and this sprung open the bones that I mentioned in such a way that
you could actually look down into the skull cavity itself and see that probably
a third or so, at least, of the brain tissue, posterior cerebral tissue and some
of the cerebellar tissue had been blasted out. There was a large amount of
bleeding which was occurring mainly from the large venous channels in the skull
which had been blasted open.
***
Mr. SPECTER. What were your initial impressions?
Dr. McCLELLAND. The initial impression that we had was that perhaps the wound in
the neck, the anterior part of the neck, was an entrance wound and that it had
perhaps taken a trajectory off the anterior vertebral body and again into the
skull itself, exiting out the back, to produce the massive injury in the head.
However, this required some straining of the imagination to imagine that this
would happen, and it was much easier to explain the apparent trajectory by means
of two bullets, which we later found out apparently had been fired, than by just
one then, on which basis we were originally taking to explain it.
Mr. SPECTER. Through the use of the pronoun "we" in your last answer, to whom do
you mean by "we"?
Dr. McCLELLAND. Essentially all of the doctors that have previously been
mentioned here.
Mr. SPECTER. Did you observe the condition of the back of the President's head ?
Dr. McCLELLAND. Well, partially; not, of course, as I say, we did not lift his
head up since it was so greatly damaged. We attempted to avoid moving him any
more than it was absolutely necessary, but I could see, of course, all the
extent of the wound.
Mr. SPECTER. You saw a large opening which you have already described?
Dr. McCLELLAND. I saw the large opening which I have described.
Mr. SPECTER. Did you observe any other wound on the back of the head?
Dr. McCLELLAND. No.
Mr. SPECTER. Did you observe a small gunshot wound below the large opening on
the back of the head ?
Dr. McCLELLAND. No.
▲
▲
Dr. Malcolm Oliver Perry, physician and surgeon:
Mr. SPECTER. Will you continue, then, Dr. Perry, as to what you observed of his
condition?
Dr. PERRY. Yes, there was blood noted on the carriage and
a large avulsive wound
on the right posterior cranium. I cannot state the size, I did not examine it at
all. I just noted the presence of lacerated brain tissue. In the lower part of
the neck below the Adams apple was a small, roughly circular wound of perhaps 5
mm. in diameter from which blood was exuding slowly. I did not see any other
wounds.
***
Mr. SPECTER. Will you now describe as specifically as you can, the injury which
you noted in the President's head?
Dr. PERRY. As I mentioned previously in the record, I made only a cursory
examination of the President's head. I noted a large avulsive wound of the right
parietal occipital area, in which both scalp and portions of skull were absent,
and there was severe laceration of underlying brain tissue. My examination did
not go any further than that.
Mr. SPECTER. Did you, to be specific, observe a smaller wound below the large
avulsed area which you have described?
Dr. PERRY. I did not.
***
Mr. SPECTER. Did you observe any wound in the President's chest?
Dr. PERRY. I did not.
Mr. SPECTER. Did you observe any wound on the left side of the President's head?
Dr. PERRY. No, sir.
▲
▲
Dr. Paul Conrad Peters, Doctor of medicine:
Mr. SPECTER What did you observe as to the nature of the President's wound?
Dr. PETERS. Well, as I mentioned, the neck wound had already been interfered
with by the tracheotomy at the time I got there, but I noticed the head wound,
and as I remember--I noticed that there was a large defect in the occiput.
Mr. SPECTER What did you notice in the occiput?
Dr. PETERS.
It seemed to me that in the right
occipitalparietal area that there was a large defect. There appeared to be bone loss and brain loss in the area.
Mr. SPECTER. Did you notice any holes below the occiput, say, in this area below
here?
Dr. PETERS. No, I did not and at the time and the moments immediately following
the injury, we speculated as to whether he had been shot once or twice because
we saw the wound of entry in the throat and noted the large occipital wound, and
it is a known fact that high velocity missiles often have a small wound of
entrance and a large wound of exit, and I'm just giving you my honest
impressions at the time.
Mr. SPECTER. What were they?
Dr. PETERS. Well, I wondered whether or not he had been shot once or twice that
was my question at the time.
Mr. SPECTER. When you say "we speculate," whom do you mean by that?
Dr. PETERS. Well, the doctors in attendance there.
Mr. SPECTER. Any doctor specifically?
Dr. PETERS. I wouldn't mention anyone specifically, we all discussed it. I did
not know whether or not he had been shot once or twice.
Dr. Kenneth Everett Salyer,
Physician:
Mr. SPECTER. What did you observe with respect to the head wound?
Dr. SALYER. I came in on the left side of him and noticed that his major wound
seemed to be in his right temporal area, at least from the point of view that I
could see him, and other than that--nothing other than he did have a gaping
scalp wound-- cranial wound.
Full Text available on the [JFK LINKS] Page (Parkland Hospital)
HEAD SHOT PHOTO CLOSE UP JFK ZAPRUDER FLIM FRAME WOUND DALLAS DOCTORS.
wounds injury head shot treatment medical evidence jfk kennedy assassination
autopsy rreport what really happened BACK AND TO THE LEFT.
HEADSHOT PHOTOGRAPH WOUND DALLAS DOCTORS JFK ASSASSINATION SECOND
SHOOTER.
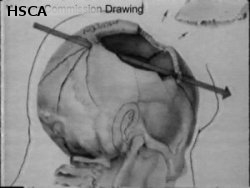
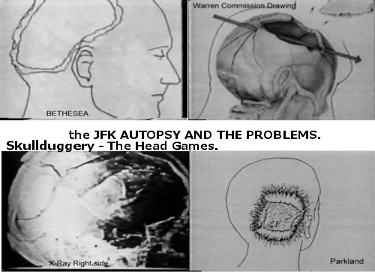
the AUTOPSY
SECTION. and the Headshot.
The back of his head....Well, it was very bad---you
know.
JFK ASSASSINATION
[
HOME ]
![]() the GRAND SUBVERSION.
the GRAND SUBVERSION.
PRESIDENT JOHN F KENNEDY JFK AUTOPSY REPORT WARREN REPORT.
SINGLE BULLET THEORY SECTION.
PARKLAND HOSPITAL,
THROAT-NECK WOUND
medical Description:
Dr.
Akin -
Dr.
Bashour -
Dr.
Baxter -
Dr.
Carrico -
Dr.
Clark - Nurse
Henchliffe -
Dr.
Jenkins - Dr.
Jones
- Dr.
McClelland - Dr.
Perry
- Dr.
Salyer
▲
Parkland Hospital Dallas Doctors, JFK
Assassination:
![]() [
BACK
] JFK Autopsy Page ( 3 )
[
BACK
] JFK Autopsy Page ( 3 )
DR. Gene Coleman Akin, Anesthesiology.:
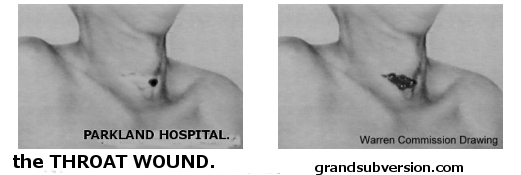
"There was a midline neck wound below the level of the cricoid cartilage,
about
1 to 1.5 cm. in diameter, the lower part of this had been cut across when I saw
the wound, it had been cut across with a knife in the performance of the
tracheotomy."
Mr. SPECTER. And as to the neck wound, did you have
occasion to observe whether there was a smooth, jagged, or what was the nature of the portion of the neck
wound which had not been cut by the tracheotomy?
Dr. AKIN. "It was slightly ragged around the edges."
Dr. Fouad Bashour, cardiology
Mr. SPECTER.: Did you have an opportunity to see the neck wound before the
tracheotomy was performed?
Dr. BASHOUR. No; I came after everything was done to him.
Dr. Charles Rufus Baxter, general surgeon:
"The wound on the neck was approximately an inch and a haft above the manubrium
of the sternum, the sternal notch. This wound
was in my estimation, 4 to 5 mm. in widest diameter and was a spherical wound. The edges of it--the size of the
wound is measured by the hole plus the damaged skin around the area, so that it
was a very small wound."
▲
▲
Dr. Charles James Carrico, surgery:
Mr. SPECTER. Will you describe, as specifically as you can then, the neck wounds
which you heretofore mentioned briefly?
Dr. CARRICO. There
was a
small wound, 5- to 8-mm. in size, located in the lower
third of the neck, below the thyroid cartilage,
the Adams apple.
Mr. DULLES. Will you show us about where it was?
Dr. CARRICO. Just about where your tie would be.
Mr. DULLES. Where did it enter?
Dr. CARRICO.
It entered?
Mr. DULLES. Yes.
Dr. CARRICO. At the time we did not know
Mr. DULLES. I see.
Dr. CARRICO. The entrance. All we knew this was a small wound here.
Mr. DULLES. I see. And you put your hand right above where your tie is?
Dr. CARRICO. Yes, sir; just where the tie--
Mr. DULLES. A little bit to the left.
Dr. CARRICO. To the right.
Mr. DULLES. Yes; to the right.
Dr. CARRICO. Yes. And this wound was fairly round, had no jagged edges, no
evidence of powder burns, and so forth.
Dr. William Kemp Clark, neurological Surgeon:
***
Dr. CLARK. I remember using the phrase to describe the location of a wound in
the President's throat as being at the point of his knot of his necktie. I do
not recall ever specifically stating that this was an entrance wound, as has
been said before. I was not present when the President arrived and did not see
this wound. If any statement regarding its entrance or exit was made by me, it
was indicating that there was a small wound described there by the physicians
who first saw the President.
▲
▲
Margaret M. Henchliffe, nurse:
Mr. SPECTER. Did you see any wound on any other part of his body?
Miss HENCHLIFFE. Yes; in the neck.
Mr. SPECTER. Will you describe it, please?
Miss HENCHLIFFE. It was just a little hole in the middle of his neck.
Mr. SPECTER. About how big a hole was it?
Miss HENCHLIFFE.
About as big around as the end of my little finger.
Mr. SPECTER. Have you ever had any experience with bullet holes?
Miss HENCHLIFFE. Yes.
Mr. SPECTER. And what did that appear to you to be?
Miss HENCHLIFFE. An entrance bullet hole it looked to me like.
Mr. SPECTER. Could it have been an exit bullet hole?
Miss HENCHLIFFE. I have never seen an exit bullet hole I don't remember seeing
one that looked like that.
Mr. SPECTER. What were the characteristics of the hole?
Miss HENCHLIFFE. It was just a little round---just a little round hole, just a
little round jagged-looking---jagged a little bit.
Mr. SPECTER. What experience have you had in observing bullet holes, Miss
Henchliffe?
Miss HENCHLIFFE. Well, we take care of a lot of bullet wounds down there--I
don't know how many a year.
Mr. SPECTER. Have you ever had any formal studies of bullet holes?
Miss HENCHLIFFE. Oh, no; nothing except my experience in the emergency room.
Mr. SPECTER. In what?
Miss HENCHLIFFE. In the emergency room is all.
***
(In approximately 3 minutes thereafter the witness returned to the deposing room
and the deposition continued as follows:)
Mr. SPECTER. Let me ask you a couple of questions more, Miss Henchliffe, one
other question, or two, before you go.
Was the wound on the front of the neck surrounded by any blood?
Miss HENCHLIFFE. No, sir.
Mr. SPECTER. Was there any blood at all in that area?
Miss HENCHLIFFE. No, sir.
Mr. SPECTER. What was there about the wound, if you recall anything special,
which gave you the impression it was an entrance wound?
Miss HENCHLIFFE.
Well, it was just a small wound and
wasn't jagged like most of the exit bullet wounds that
I have seen.
Mr. SPECTER. If there was a high-powered rifle, or a high-powered rifle was
going at a fast speed, as fast as 2,000 feet per second, which encountered only
soft tissue in the body, would you have sufficient knowledge to know whether or
not the appearance of that hole would be consistent with an exit wound?
Miss HENCHLIFFE. Well, from some information I received in talking to someone
about guns later on, they said that this is possible. But you have a small exit
wound---you could have a small exit wound.
▲
▲
Dr. Marion Thomas Jenkins, Anesthesiology:
Mr. SPECTER Would you describe that wound as specifically as you can?
Dr. JENKINS. Well, I'm afraid my description of it would not be as accurate, of
course, as that of the surgeons who were doing the tracheotomy, because my look
was a quick look before connecting up the endotracheal tube to the apparatus to
help in ventilation and respiration for the patient, and I was aware later in
the day, as I should have put it in the report, that I thought this was a wound
of exit because it was not a clean wound, and by "clean" clearly demarcated,
round, punctate wound which is the usual wound of an entrance wound, made by a
missile and at some speed. Of course, entrance wounds with a lobbing type
missile, can make a jagged wound also, but I was of the impression and I
recognized
I had the impression it was an exit wound. However, my mental
appreciation for a wound--for the wound in the neck, I believe, was sort of--was
overshadowed by recognition of the wound in the scalp and skull plate.
Dr. Ronald Coy Jones, General Surgery:
Mr. SPECTER. Did you observe any wounds ?
Dr. JONES. As we saw him the first time, we noticed that he had a small wound at
the midline of the neck, just above the superasternal notch, and this was
probably no greater than a quarter of an inch in greatest diameter, and that he
had a large wound in the right posterior side of the head.
Mr. SPECTER. When you say "we noticed," whom do you mean by that?
Dr. JONES. Well, Dr. Perry and I were the two that were there at this time
observing.
Mr. SPECTER. Did Dr. Perry make any comment about the nature of the wound at
that time? Either wound?
Dr. JONES. Not that I recall.
***
Mr. SPECTER. Will you describe as precisely as you can the wound that you
observed in the throat ?
Dr. JONES. The wound in the throat was probably no larger than a quarter of an
inch in diameter. There appeared to be no powder burn present, although this
could have been masked by the amount of blood that was on the head and neck,
although there was no obvious, amount of powder present. There appeared to be a
very minimal amount of disruption of interruption of the surrounding skin.
There
appeared to be
relatively smooth edges around the wound, and if this occurred as
a result of a missile, you would have probably thought it was a missile of very
low velocity and probably could have been compatible with a bone fragment of
either--probably exiting from the neck,
but it was a very small, smooth wound.
Mr. SPECTER. Did you notice any lump in the throat area ?
Dr. JONES. No; I didn't.
Mr. SPECTER. Was there any blood on the throat area in the vicinity of the wound
which you have described of the throat?
Dr. JONES. Not a great deal of blood, as if in relation to the amount that was
around the head--not too much.
***
Mr. SPECTER. Dr. Jones, I now hand you a report which purports to bear your
signature, labeled "Summary of treatment of the President," dated November 23,
1963, which I shall now ask the Court Reporter to mark as Dr. Jones' Exhibit No.
1.
(Instrument mentioned marked by the Reporter as Dr. Jones' Exhibit No. 1, for
identification.)
Mr. SPECTER. I ask you if this in fact is your signature ?
Dr. JONES. Yes.
Mr. SPECTER. And I ask you if this was the report which you submitted concerning
your participation of the treatment of President Kennedy?
Dr. JONES. Yes; it was.
Mr. SPECTER. In this report, Dr. Jones, you state the following, "Previously
described severe skull and brain injury was noted as well as a small hole in
anterior midline of the neck thought to be a bullet entrance wound. What led you
to the thought that it was a bullet entrance wound, sir?
Dr. JONES. The hole was very small and relatively clean cut, as you would see in
a bullet that is entering rather than exiting from a patient. If this were an
exit wound, you would think that it exited at a very low velocity to produce no
more damage than this had done, and if this were a missile of high velocity, you
would expect more of an explosive type of exit wound, with more tissue
destruction than this appeared to have on superficial examination.
Mr. SPECTER. Would it be consistent, then, with an exit wound, but of low
velocity, as you put it?
Dr. JONES. Yes; of very low velocity to the point that you might think that this
bullet barely made it through the soft tissues and just enough to drop out of
the skin on the opposite side
▲
▲
Dr. Robert Nelson McClelland,
general surgery:
Dr. McCLELLAND. The neck wound, when I first arrived, was at this time converted
into a tracheotomy incision. The skin incision had been made by Dr. Perry, and
he told me---although I did not see that---that he had made the incision through
a very small, perhaps less than one quarter inch in diameter wound in the neck.
Mr. SPECTER. Do you recall whether he described it any more precisely than that?
Dr. McCLELLAND. He did not at that time.
Mr. SPECTER. Has he ever described it any more precisely for you?
Dr. McCLELLAND. He has since that time.
Mr. SPECTER. And what description has he given of it since that time?
Dr. MCCLELLAND. As well as I can recall, the description that he gave was
essentially as I have just described, that it was a very small injury, with
clear cut, although somewhat irregular margins of less than a quarter inch in
diameter, with minimal tissue damage surrounding it on the skin.
Mr. SPECTER. Now, was there anything left for you to observe of that bullet
wound, or had the incision obliterated it?
Dr. McCLELLAND. The incision had obliterated it, essentially, the skin portion,
that is.
***
Mr. SPECTER. Based on the experience that you have described for us with gunshot
wounds and your general medical experience, would you characterize the
description of the wound that Dr. Perry gave you as being a wound of entrance or
a wound of exit, or was the description which you got from Dr. Perry and Dr.
Baxter and Dr. Carrico who were there before, equally consistent with whether or
not it was a wound of entrance or a wound of exit, or how would you characterize
it in your words?
Dr. McCLELLAND. I would say it would be equally consistent with either type
wound, either an entrance or an exit type wound. It would be quite difficult to
say--impossible.
▲
▲
Dr. Malcolm Oliver Perry, physician and surgeon:
Mr. SPECTER. Will you continue, then, Dr. Perry, as to what you observed of his
condition?
Dr. PERRY. Yes, there was blood noted on the carriage and a large avulsive wound
on the right posterior cranium. I cannot state the size, I did not examine it at
all. I just noted the presence of lacerated brain tissue.
In the lower part of
the neck below the Adams apple was a small, roughly circular wound of
perhaps 5
mm. in diameter from which blood was exuding slowly. I did not see any other
wounds.
***
Mr. SPECTER. Why did you elect to make the tracheotomy incision through the
wound in the neck, Dr. Perry?
Dr. PERRY. The area of the wound, as pointed out to you in the lower third of
the neck anteriorly is customarily the spot one would electively perform the
tracheotomy. This is one of the safest and easiest spots to reach the trachea.
In addition the presence of the wound indicated to me there was possibly an
underlaying wound to the neck muscles in the neck, the carotid artery or the
jugular vein. If you are going to control these it is necessary that the
incision be as low, that is toward the heart or lungs as the wound if you are
going to obtain adequate control. Therefore, for expediency's sake I went
directly to that level to obtai control of the airway.
***
Mr. SPECTER. Dr. Perry, you mentioned an injury to the trachea. Will you
describe that as precisely as you can, please?
Dr. PERRY. Yes. Once the transverse incision through the skin and subcutaneous
tissues was made, it was necessary to separate the strap muscles covering the
anterior muscles of the windpipe and thyroid. At that point the trachea was
noted to be deviated slightly to the left and I found it necessary to sever the
exterior strap muscles on the other side to reach the trachea. I noticed a small
ragged laceration of the trachea on the anterior lateral right side. I could see
the endotracheal tube which had been placed by Dr. Carrico in the wound, but
there was evidence of air and blood around the tube because I noted the cuff was
just above the injury to the trachea.
***
Mr. SPECTER. Would you now describe as particularly as possible the neck wound
you observed?
Dr. PERRY. This was situated in the lower anterior one-third of the neck,
approximately 5 mm. in diameter. It was exuding blood slowly which partially
obscured it. Its edges were neither ragged nor were they punched out, but rather
clean.
Mr. SPECTER. Have you now described the neck wound as specifically as you can?
Dr. PERRY. I have.
Mr. SPECTER. Based on your observations of the neck wound alone, do you have a
sufficient basis to form an opinion as to whether it was an entrance wound or an
exit wound.
Dr. PERRY. No, sir. I was unable to determine that since
I did not ascertain the
exact trajectory of the missile. The operative procedure which I performed was
restricted to securing an adequate airway and insuring there was no injury to
the carotid artery or jugular vein at that level and at that point I made the
procedure.
Mr. SPECTER. Based
on the appearance of the neck wound alone,
could it have been either an entrance or an exit
wound?
Dr. PERRY. It could have been either.
▲
▲
Dr. Kenneth Everett Salyer, Physician:
Mr. SPECTER. I had asked you a moment ago whether you had an opportunity to
observe the condition of the President's throat.
Dr. SALYER. Right.
Mr. SPECTER. What was your answer to that question?
Dr. SALYER The answer was--there were a lot of doctors standing around, and I
didn't really get to observe the nature of the wound in the throat.
▲
▲
Full Text available on the [JFK
LINKS] Page (Parkland Hospital)
President John F Kennedy JFK Assassination Wound
throat back head injury shot treatment gunshots medical autopsy report evidence who killed him the TRUTH.

jfk throat neck wound head injury john f kennedy autopsy report shot single bullet path autopsy
doctors photo footage description of.
JFK
ASSASSINATION [
HOME ]
![]() the GRAND SUBVERSION.
the GRAND SUBVERSION.
|
Page Subject : List of External Links. |
||
| Autopsy Report.jfk | ||
|
|
||
![]() [
BACK
] JFK Autopsy Page ( 3 )
[
BACK
] JFK Autopsy Page ( 3 )
grandsubversion.com:
SECTION:
[Parkland Hospital]--[Bethesda
Autopsy]--[Dallas I]--[Dallas
II]--[Shots]--[Magic
Single Bullet Theory]--[Oswald
I]--[Oswald II]--[Oswald
III]--[Oswald
IV]--[Three
Tramps]--[Dallas
Police]
| grandsubversions.com NEW Grassy Knoll ENHANCEMENTS. | |||
| Moorman photo. | Black Dog Image. | Knoll Overview. | Gordon Arnold Factor. |
 |
 |
 |
 |
| CLICK IMAGE FOR ENHANCEMENT PAGE. |
 jfk assassination Kennedy photo Dallas doctors autopsy report parkland hospital description wounds. GRANDSUBVERSIONS JFK AUTOPSY PAGE (1) CONSPIRACY OR SIMPLE MISTAKES? |
The jfk Neck Head and Throat Wound description medical BEFORE AND AFTER. |
PRESIDENT JOHN F KENNEDY JFK AUTOPSY REPORT
GUN SHOT WOUND INJURY CONSPIRACY PHOTO IMAGE PICTURE ASSASSNIATION 2018 2019
2020.

JFK Assassination death photos John f kennedy car
the JFK ASSASSINATION CONSPIRACY HOME the GRAND SUBVERSION.

HEADSHOT JFK ASSASSINATION KENNEDY WOUNDS GUNSHOTS ZAPRUDER FILM FOOTAGE
CONSPIRACY THEORIES PHOTOS PICTURES.

JFK ASSASSINATION JOHN F KENNEDY ROBERT JR MLK AUTOPSY REPORT BRAIN HEAD SHOT
CONSPIRACY THEORIES.
JFK ASSASSINATION
[
HOME ]
![]() the GRAND SUBVERSION.
the GRAND SUBVERSION.